
Connection Between Stress and Stroke: The Hidden Risk Factor
Stroke remains a leading cause of mortality and disability worldwide, with over 15 million cases annually claiming nearly 6 million lives. While healthcare professionals traditionally focus on well-established risk factors—hypertension, diabetes, smoking, and high cholesterol—an often-overlooked yet scientifically validated contributor lurks behind the scenes: stress and psychological distress. This comprehensive article explores the intricate connection between stress and stroke, examining the biological mechanisms that transform emotional tension into cerebrovascular catastrophe, and provides evidence-based strategies for mitigation.
The relationship between stress and stroke is not merely correlational; mounting clinical and experimental evidence demonstrates that psychological stress operates as an independent, modifiable risk factor capable of triggering acute cerebrovascular events or, over time, fundamentally altering the brain's vascular architecture. Understanding this connection empowers both healthcare providers and patients to implement preventive interventions that address this underrecognized dimension of stroke risk.
How Stress Increases Stroke Risk: The Biological Mechanisms
The human body's stress response system, while evolutionarily adaptive for short-term survival threats, becomes pathogenic when activated chronically or excessively. Multiple interconnected physiological pathways explain how stress translates into stroke vulnerability.
How Chronic Stress Increases the Risk of Stroke
When we experience stress, our bodies react to protect us. However, when stress becomes a constant, everyday occurrence, it physically changes our bodies in ways that greatly increase the risk of having a stroke and make recovering from one much harder. Here is exactly how stress breaks down our bodily systems:
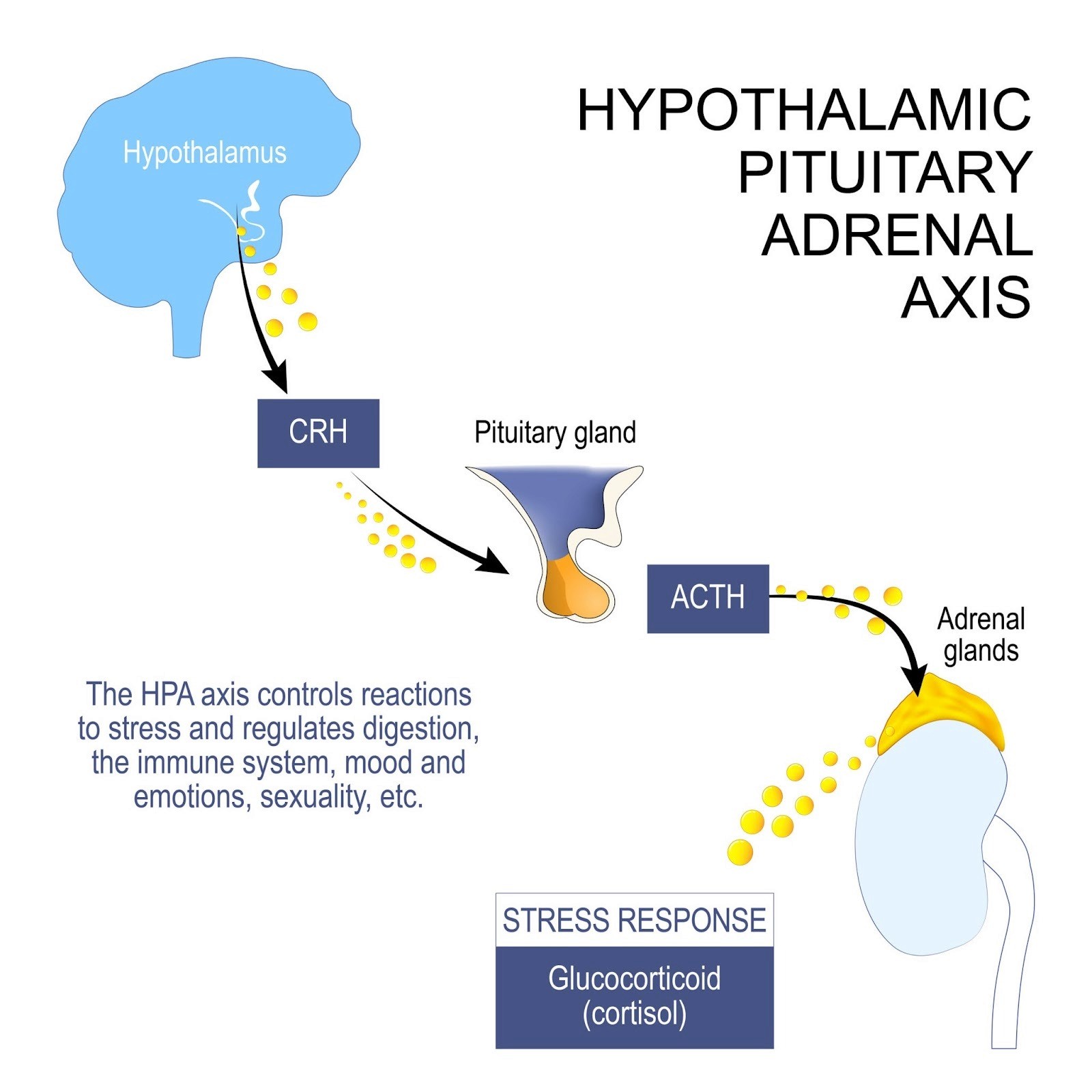
1. The Stress Hormone Overload (Cortisol)
When your brain senses a threat, it triggers a chain reaction that floods your body with cortisol, the primary stress hormone.
2. Damaged Blood Vessel Linings (Endothelial Dysfunction)
Your blood vessels are lined with a delicate, single layer of cells called the endothelium, which acts like a smart control center for blood flow.
Constant stress damages this lining. It stops producing the chemicals needed to keep blood vessels relaxed and flexible.
As a result, healthy, stretchy blood vessels become stiff, damaged, and prone to blockages, which is the primary cause of a stroke.
3. Blood Pressure Spikes and the "Fight or Flight" Response
Stress triggers your adrenal glands to release adrenaline, making your heart beat faster and your blood pressure rise.
Over time, chronic stress trains your body to overreact. Even minor everyday frustrations can cause massive spikes in your blood pressure.
This exaggerated reaction is a huge warning sign. Men who experience extreme blood pressure spikes during minor stress tests have an 87% higher risk of suffering a stroke. This risk is even higher for people facing financial or social hardships.
4. Inflammation and Artery Plaque (Atherosclerosis)
You might think of stress as purely mental, but it causes physical inflammation in your bloodstream.
Sudden mental stress pushes inflammatory cells into the walls of your blood vessels.
Long-term stress is even worse: it tricks your bone marrow into mass-producing inflammatory cells. These cells build up inside your arteries as "plaque," clogging them up much faster than normal.
5. Power Failures in Brain Cells (Mitochondria)
Mitochondria are the tiny "batteries" inside your cells that produce energy.
Chronic stress damages these batteries.
If a stroke happens, your brain cells desperately need energy to repair themselves and survive the lack of blood flow. Because stress has already damaged their power source, the brain cells die off much faster, making the stroke's impact far worse.
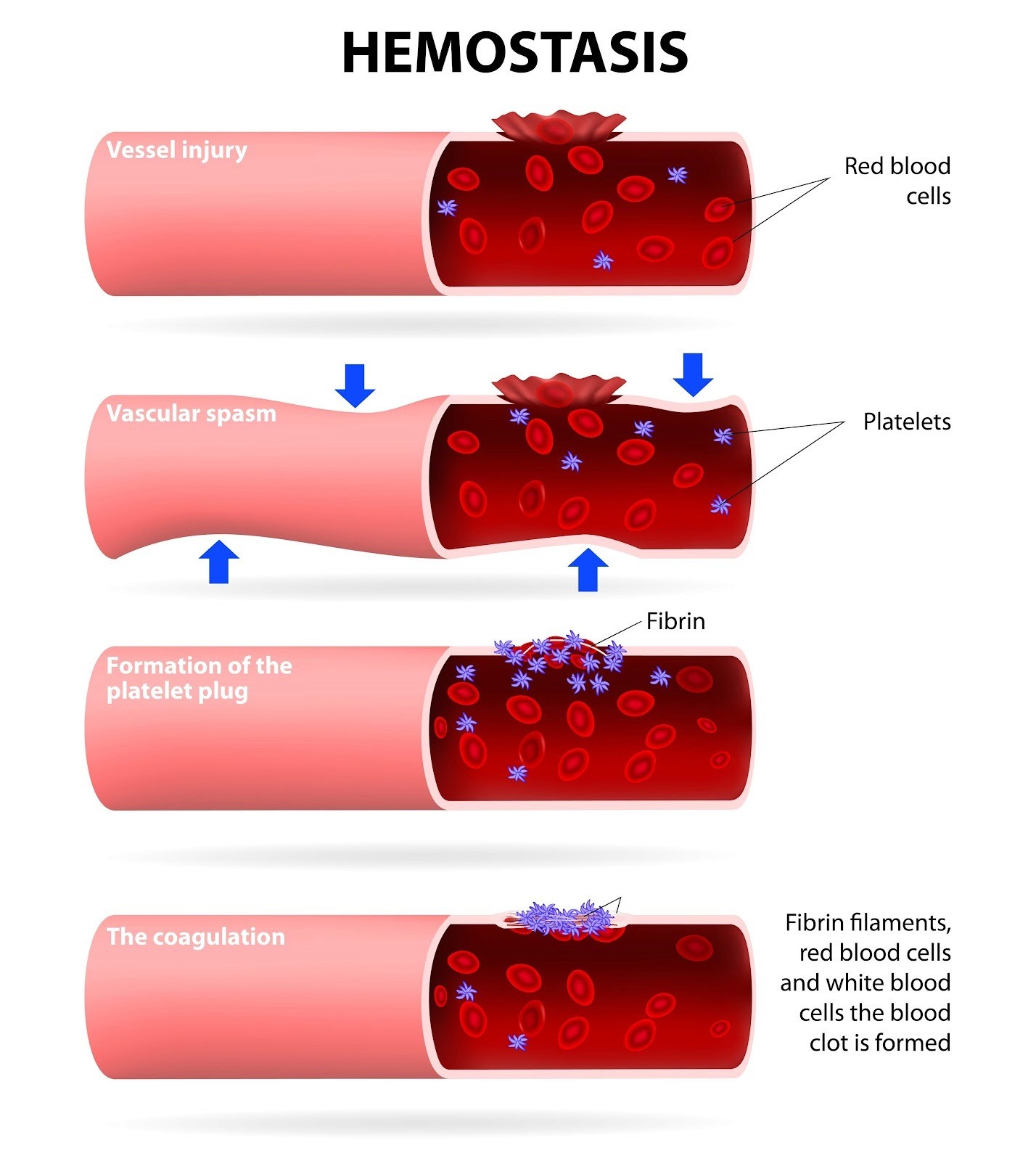
6. "Sticky" Blood and Clotting
Finally, constant stress changes the actual makeup of your blood.
Epidemiological Evidence: The Magnitude of Risk
Clinical evidence corroborates these mechanistic insights. A large international case-control study of 26,812 participants with first-ever stroke found that self-reported psychosocial stress within the preceding 12 months was associated with increased stroke risk across all stress domains. Several periods of work stress or permanent work stress conferred a 2.70-fold increased odds of all stroke types, with particularly strong associations for hemorrhagic stroke (odds ratio 5.20). Remarkably, these associations persisted after adjustment for socioeconomic status, occupation, educational level, and cardiovascular risk factors, suggesting that stress operates partly through mechanisms independent of traditional risk factors.
Acute psychological stress functions as an immediate stroke trigger. A case-crossover analysis of 151 acute stroke patients identified that acute emotional stress preceded stroke onset in a substantial proportion of cases, increasing the odds of stroke in the subsequent two hours by 3.4-fold compared to stress-free periods. This acute triggering mechanism likely involves catecholamine-mediated vasospasm, plaque rupture, and arrhythmia in susceptible individuals. A US-based study utilizing the National Health Interview Survey demonstrated that psychological distress increases stroke odds by more than twofold among the general adult population, with effects intensifying in women and minority populations.
In young adults aged 18-39 years, self-perceived stress emerges as an independent predictor of cryptogenic ischemic stroke—stroke lacking identifiable conventional risk factors. This observation proves particularly important because it suggests that stress alone, through its effects on endothelial function and hemostasis, suffices to cause stroke in young individuals without atherosclerotic disease or cardiac pathology.
Ischemic Versus Hemorrhagic Stroke: Differential Associations with Stress
Stress exhibits type-specific associations with different stroke subtypes. Ischemic stroke—accounting for 85% of all cerebrovascular events—predominantly associates with chronic stress exposure. Through mechanisms of atherosclerosis acceleration, endothelial dysfunction, and prothrombotic state, chronic psychological stress creates the substrate for thrombotic or embolic stroke.
Hemorrhagic stroke, while less common (13% of all strokes), demonstrates stronger associations with acute stress. The acute catecholamine surge characteristic of intense emotional arousal elevates intracranial pressure, destabilizes intracerebral aneurysms, and disrupts autoregulation of cerebral blood vessels, predisposing to rupture. Accordingly, case studies frequently document hemorrhagic stroke occurring during or immediately after intense emotional events.
The Stress-Induced Stroke Profile: Which Patients Are Most Vulnerable?
Not all individuals exposed to stress demonstrate equal stroke risk. Several population-level and individual-level factors modify the stress-stroke association. Locus of control—the psychological construct capturing perceived ability to influence life circumstances—significantly modifies stress effects. Individuals perceiving low control at work who simultaneously experience high work stress demonstrate substantially elevated stroke risk compared to those with high perceived control. This interaction suggests that psychological appraisal of stressor manageability, not merely objective stressor exposure, determines pathophysiological impact.
Socioeconomic status represents another critical modifier. Men combining high blood pressure reactivity to stress with low education levels faced nearly 3-fold stroke risk compared to better-educated, less reactive counterparts. The accumulated burden of chronic psychosocial adversity that characterizes lower socioeconomic position—including financial insecurity, occupational strain, discrimination, and limited access to health resources—amplifies the nervous system's stress responsivity.
Age and sex influence stress-stroke relationships. Young women demonstrate stronger associations between permanent work stress and cryptogenic ischemic stroke, suggesting that reproductive hormones or sex-specific stress physiology may modulate cerebrovascular vulnerability. The emerging recognition of early-onset stroke in young professionals experiencing intense occupational pressure reflects this age-related vulnerability.
Psychiatric comorbidity compounds stress effects. Depression and anxiety disorders, which share neurobiological underpinnings with psychological stress, further dysregulate the HPA axis and autonomic nervous system, multiplying stroke risk. The finding that depression-associated genetic variants independently predict poor stroke outcomes within 90 days of onset indicates that genetically determined propensity toward mood disturbance represents an inherited vulnerability to stress-mediated stroke.
Clinical Recognition: Warning Signs and Presentation
Healthcare providers should maintain elevated suspicion for stress-triggered stroke, particularly in younger patients presenting without traditional risk factors or in individuals experiencing acute emotional turmoil preceding symptom onset. Classic acute stroke symptoms apply regardless of etiology: sudden facial weakness or numbness (especially unilateral), arm or leg weakness or numbness, speech difficulty or comprehension impairment, vision disturbance, dizziness or imbalance, and severe sudden headache. However, recognition of stress as a precipitant enables more targeted prevention strategies and facilitates psychological intervention post-stroke.
Prevention and Risk Mitigation: An Evidence-Based Framework
Since approximately 90.5% of global stroke burden is attributable to modifiable risk factors, aggressive stress management represents an underutilized prevention strategy. Multimodal intervention addressing stress alongside traditional risk factors achieves approximately 80% cumulative risk reduction in recurrent vascular events.
Lifestyle-Based Stress Management
Meditation and mindfulness practices reduce sympathetic nervous system activity, lower cortisol levels, and improve endothelial function. Regular meditation practice (15-20 minutes daily) demonstrably reduces blood pressure and inflammatory markers in hypertensive and at-risk populations.
Aerobic exercise (150 minutes moderate intensity weekly) simultaneously addresses multiple pathways: it reduces perceived stress, improves autonomic nervous system balance (increasing parasympathetic tone), reduces inflammatory markers, optimizes endothelial function, and improves insulin sensitivity. The beneficial effects extend beyond the exercise period itself; regular exercisers demonstrate blunted blood pressure and catecholamine responses to acute stressors.
Cognitive-behavioral stress management teaches individuals to reframe stressful appraisals, develop coping strategies, and increase perceived control—thereby reducing the downstream physiological cascade. Structured programs demonstrate efficacy in stroke survivors and high-risk populations.
Sleep optimization restores parasympathetic tone and normalizes HPA axis function. Sleep deprivation, conversely, increases stress hormone levels and impairs endothelial function. Targeting 7-9 hours nightly should be part of comprehensive stroke prevention.
Dietary Approaches
A Mediterranean-pattern diet rich in antioxidants, anti-inflammatory compounds, and omega-3 fatty acids directly counters the inflammatory and oxidative milieu created by chronic stress. Limiting sodium intake (to <2,300 mg daily, ideally <1,500 mg) reduces blood pressure and prevents stress-induced hypertensive surges. Restricting refined carbohydrates and added sugars prevents stress-induced hyperglycemia and maintains metabolic homeostasis.
Pharmacological Considerations
For individuals with treatment-resistant hypertension or severe anxiety disorders, pharmacotherapy becomes necessary. Beta-blockers, ACE inhibitors, and angiotensin receptor blockers independently reduce stress-related cardiovascular events while also lowering blood pressure. Selective serotonin reuptake inhibitors treat concurrent depression and anxiety while modulating stress physiology. However, pharmacotherapy should complement, not replace, lifestyle modifications.
Psychosocial Interventions
Workplace modifications reducing occupational strain—including increasing autonomy, reducing excessive demands, and fostering supportive environments—demonstrate measurable reductions in cardiovascular events. Community-level social support, peer networks, and sense of belonging buffer against the deleterious effects of chronic stress.
Conclusion
The connection between stress and stroke represents a paradigm shift in understanding cerebrovascular disease etiology. No longer can stroke be viewed as a purely vascular disorder; it emerges as a psychoneuroimmune phenomenon where emotional experience, through multiple interconnected biological pathways, fundamentally alters cerebrovascular structure and function. The evidence is unequivocal: chronic and acute psychological stress independently increases stroke risk across populations, with magnitude rivaling or exceeding traditional cardiovascular risk factors.
For healthcare professionals, this understanding necessitates systematic assessment of psychosocial stress and implementation of stress reduction strategies as core components of stroke prevention and secondary prevention programs. For patients, recognizing stress as a modifiable risk factor empowers engagement in lifestyle modifications and early intervention for mood and anxiety disorders. Future prevention paradigms must integrate stress management alongside blood pressure control, lipid management, and antiplatelet therapy, recognizing that optimal stroke prevention requires addressing both the vascular and psychological dimensions of human health.
Stroke remains a leading cause of mortality and disability worldwide, with over 15 million cases annually claiming nearly 6 million lives. While healthcare professionals traditionally focus on well-established risk factors—hypertension, diabetes, smoking, and high cholesterol—an often-overlooked yet scientifically validated contributor lurks behind the scenes: stress and psychological distress. This comprehensive article explores the intricate connection between stress and stroke, examining the biological mechanisms that transform emotional tension into cerebrovascular catastrophe, and provides evidence-based strategies for mitigation.
The relationship between stress and stroke is not merely correlational; mounting clinical and experimental evidence demonstrates that psychological stress operates as an independent, modifiable risk factor capable of triggering acute cerebrovascular events or, over time, fundamentally altering the brain's vascular architecture. Understanding this connection empowers both healthcare providers and patients to implement preventive interventions that address this underrecognized dimension of stroke risk.
How Stress Increases Stroke Risk: The Biological Mechanisms
The human body's stress response system, while evolutionarily adaptive for short-term survival threats, becomes pathogenic when activated chronically or excessively. Multiple interconnected physiological pathways explain how stress translates into stroke vulnerability.
How Chronic Stress Increases the Risk of Stroke
When we experience stress, our bodies react to protect us. However, when stress becomes a constant, everyday occurrence, it physically changes our bodies in ways that greatly increase the risk of having a stroke and make recovering from one much harder. Here is exactly how stress breaks down our bodily systems:
1. The Stress Hormone Overload (Cortisol)
When your brain senses a threat, it triggers a chain reaction that floods your body with cortisol, the primary stress hormone.
2. Damaged Blood Vessel Linings (Endothelial Dysfunction)
Your blood vessels are lined with a delicate, single layer of cells called the endothelium, which acts like a smart control center for blood flow.
Constant stress damages this lining. It stops producing the chemicals needed to keep blood vessels relaxed and flexible.
As a result, healthy, stretchy blood vessels become stiff, damaged, and prone to blockages, which is the primary cause of a stroke.
3. Blood Pressure Spikes and the "Fight or Flight" Response
Stress triggers your adrenal glands to release adrenaline, making your heart beat faster and your blood pressure rise.
Over time, chronic stress trains your body to overreact. Even minor everyday frustrations can cause massive spikes in your blood pressure.
This exaggerated reaction is a huge warning sign. Men who experience extreme blood pressure spikes during minor stress tests have an 87% higher risk of suffering a stroke. This risk is even higher for people facing financial or social hardships.
4. Inflammation and Artery Plaque (Atherosclerosis)
You might think of stress as purely mental, but it causes physical inflammation in your bloodstream.
Sudden mental stress pushes inflammatory cells into the walls of your blood vessels.
Long-term stress is even worse: it tricks your bone marrow into mass-producing inflammatory cells. These cells build up inside your arteries as "plaque," clogging them up much faster than normal.
5. Power Failures in Brain Cells (Mitochondria)
Mitochondria are the tiny "batteries" inside your cells that produce energy.
Chronic stress damages these batteries.
If a stroke happens, your brain cells desperately need energy to repair themselves and survive the lack of blood flow. Because stress has already damaged their power source, the brain cells die off much faster, making the stroke's impact far worse.
6. "Sticky" Blood and Clotting
Finally, constant stress changes the actual makeup of your blood.
Epidemiological Evidence: The Magnitude of Risk
Clinical evidence corroborates these mechanistic insights. A large international case-control study of 26,812 participants with first-ever stroke found that self-reported psychosocial stress within the preceding 12 months was associated with increased stroke risk across all stress domains. Several periods of work stress or permanent work stress conferred a 2.70-fold increased odds of all stroke types, with particularly strong associations for hemorrhagic stroke (odds ratio 5.20). Remarkably, these associations persisted after adjustment for socioeconomic status, occupation, educational level, and cardiovascular risk factors, suggesting that stress operates partly through mechanisms independent of traditional risk factors.
Acute psychological stress functions as an immediate stroke trigger. A case-crossover analysis of 151 acute stroke patients identified that acute emotional stress preceded stroke onset in a substantial proportion of cases, increasing the odds of stroke in the subsequent two hours by 3.4-fold compared to stress-free periods. This acute triggering mechanism likely involves catecholamine-mediated vasospasm, plaque rupture, and arrhythmia in susceptible individuals. A US-based study utilizing the National Health Interview Survey demonstrated that psychological distress increases stroke odds by more than twofold among the general adult population, with effects intensifying in women and minority populations.
In young adults aged 18-39 years, self-perceived stress emerges as an independent predictor of cryptogenic ischemic stroke—stroke lacking identifiable conventional risk factors. This observation proves particularly important because it suggests that stress alone, through its effects on endothelial function and hemostasis, suffices to cause stroke in young individuals without atherosclerotic disease or cardiac pathology.
Ischemic Versus Hemorrhagic Stroke: Differential Associations with Stress
Stress exhibits type-specific associations with different stroke subtypes. Ischemic stroke—accounting for 85% of all cerebrovascular events—predominantly associates with chronic stress exposure. Through mechanisms of atherosclerosis acceleration, endothelial dysfunction, and prothrombotic state, chronic psychological stress creates the substrate for thrombotic or embolic stroke.
Hemorrhagic stroke, while less common (13% of all strokes), demonstrates stronger associations with acute stress. The acute catecholamine surge characteristic of intense emotional arousal elevates intracranial pressure, destabilizes intracerebral aneurysms, and disrupts autoregulation of cerebral blood vessels, predisposing to rupture. Accordingly, case studies frequently document hemorrhagic stroke occurring during or immediately after intense emotional events.
The Stress-Induced Stroke Profile: Which Patients Are Most Vulnerable?
Not all individuals exposed to stress demonstrate equal stroke risk. Several population-level and individual-level factors modify the stress-stroke association. Locus of control—the psychological construct capturing perceived ability to influence life circumstances—significantly modifies stress effects. Individuals perceiving low control at work who simultaneously experience high work stress demonstrate substantially elevated stroke risk compared to those with high perceived control. This interaction suggests that psychological appraisal of stressor manageability, not merely objective stressor exposure, determines pathophysiological impact.
Socioeconomic status represents another critical modifier. Men combining high blood pressure reactivity to stress with low education levels faced nearly 3-fold stroke risk compared to better-educated, less reactive counterparts. The accumulated burden of chronic psychosocial adversity that characterizes lower socioeconomic position—including financial insecurity, occupational strain, discrimination, and limited access to health resources—amplifies the nervous system's stress responsivity.
Age and sex influence stress-stroke relationships. Young women demonstrate stronger associations between permanent work stress and cryptogenic ischemic stroke, suggesting that reproductive hormones or sex-specific stress physiology may modulate cerebrovascular vulnerability. The emerging recognition of early-onset stroke in young professionals experiencing intense occupational pressure reflects this age-related vulnerability.
Psychiatric comorbidity compounds stress effects. Depression and anxiety disorders, which share neurobiological underpinnings with psychological stress, further dysregulate the HPA axis and autonomic nervous system, multiplying stroke risk. The finding that depression-associated genetic variants independently predict poor stroke outcomes within 90 days of onset indicates that genetically determined propensity toward mood disturbance represents an inherited vulnerability to stress-mediated stroke.
Clinical Recognition: Warning Signs and Presentation
Healthcare providers should maintain elevated suspicion for stress-triggered stroke, particularly in younger patients presenting without traditional risk factors or in individuals experiencing acute emotional turmoil preceding symptom onset. Classic acute stroke symptoms apply regardless of etiology: sudden facial weakness or numbness (especially unilateral), arm or leg weakness or numbness, speech difficulty or comprehension impairment, vision disturbance, dizziness or imbalance, and severe sudden headache. However, recognition of stress as a precipitant enables more targeted prevention strategies and facilitates psychological intervention post-stroke.
Prevention and Risk Mitigation: An Evidence-Based Framework
Since approximately 90.5% of global stroke burden is attributable to modifiable risk factors, aggressive stress management represents an underutilized prevention strategy. Multimodal intervention addressing stress alongside traditional risk factors achieves approximately 80% cumulative risk reduction in recurrent vascular events.
Lifestyle-Based Stress Management
Meditation and mindfulness practices reduce sympathetic nervous system activity, lower cortisol levels, and improve endothelial function. Regular meditation practice (15-20 minutes daily) demonstrably reduces blood pressure and inflammatory markers in hypertensive and at-risk populations.
Aerobic exercise (150 minutes moderate intensity weekly) simultaneously addresses multiple pathways: it reduces perceived stress, improves autonomic nervous system balance (increasing parasympathetic tone), reduces inflammatory markers, optimizes endothelial function, and improves insulin sensitivity. The beneficial effects extend beyond the exercise period itself; regular exercisers demonstrate blunted blood pressure and catecholamine responses to acute stressors.
Cognitive-behavioral stress management teaches individuals to reframe stressful appraisals, develop coping strategies, and increase perceived control—thereby reducing the downstream physiological cascade. Structured programs demonstrate efficacy in stroke survivors and high-risk populations.
Sleep optimization restores parasympathetic tone and normalizes HPA axis function. Sleep deprivation, conversely, increases stress hormone levels and impairs endothelial function. Targeting 7-9 hours nightly should be part of comprehensive stroke prevention.
Dietary Approaches
A Mediterranean-pattern diet rich in antioxidants, anti-inflammatory compounds, and omega-3 fatty acids directly counters the inflammatory and oxidative milieu created by chronic stress. Limiting sodium intake (to <2,300 mg daily, ideally <1,500 mg) reduces blood pressure and prevents stress-induced hypertensive surges. Restricting refined carbohydrates and added sugars prevents stress-induced hyperglycemia and maintains metabolic homeostasis.
Pharmacological Considerations
For individuals with treatment-resistant hypertension or severe anxiety disorders, pharmacotherapy becomes necessary. Beta-blockers, ACE inhibitors, and angiotensin receptor blockers independently reduce stress-related cardiovascular events while also lowering blood pressure. Selective serotonin reuptake inhibitors treat concurrent depression and anxiety while modulating stress physiology. However, pharmacotherapy should complement, not replace, lifestyle modifications.
Psychosocial Interventions
Workplace modifications reducing occupational strain—including increasing autonomy, reducing excessive demands, and fostering supportive environments—demonstrate measurable reductions in cardiovascular events. Community-level social support, peer networks, and sense of belonging buffer against the deleterious effects of chronic stress.
Conclusion
The connection between stress and stroke represents a paradigm shift in understanding cerebrovascular disease etiology. No longer can stroke be viewed as a purely vascular disorder; it emerges as a psychoneuroimmune phenomenon where emotional experience, through multiple interconnected biological pathways, fundamentally alters cerebrovascular structure and function. The evidence is unequivocal: chronic and acute psychological stress independently increases stroke risk across populations, with magnitude rivaling or exceeding traditional cardiovascular risk factors.
For healthcare professionals, this understanding necessitates systematic assessment of psychosocial stress and implementation of stress reduction strategies as core components of stroke prevention and secondary prevention programs. For patients, recognizing stress as a modifiable risk factor empowers engagement in lifestyle modifications and early intervention for mood and anxiety disorders. Future prevention paradigms must integrate stress management alongside blood pressure control, lipid management, and antiplatelet therapy, recognizing that optimal stroke prevention requires addressing both the vascular and psychological dimensions of human health.
ಚಂದಾ ನಮ್ಮ ನ್ಯೂಸ್ಲೆಟರ್ ಗೆ
